“Now that we know where the problem is, we can improve early diagnosis and treatment in the hardest hit communities”
— Dr. Gary Doern, editor-in-chief of the journal of Clinical Microbiology, and fellow of American Academy of Microbiology and the Infectious Diseases Society of America
MRSA FAQs
What is MRSA? +
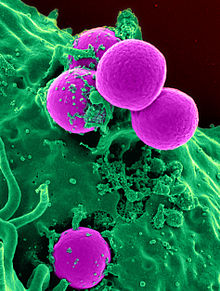
Methicillin-resistant Staphylococcus aureus, or MRSA, is a bacterium that is responsible for difficult to treat skin and other infections. Because of MRSA’s resistance to antibiotics used to kill it, MRSA is often called the “super bug.” While MRSA is usually not serious in healthy people, it can cause significant complications such as organ failure or death if it enters the bloodstream. Many survive staph infections if they are only skin deep. However, MRSA can be fatal if left untreated and becomes invasive.
Where is MRSA most prevelant? +
MRSA infections primarily originate in the community. Children who participate in contact sports, and individuals who share personal items, have a weakened immune system, live in crowded or unsanitary conditions or live below the US poverty level, are at-risk for MRSA infections. Hospital-acquired MRSA, while often not as virulent as community-acquired MRSA, still presents a serious risk. Patients who have had surgery, a lengthy ICU stay, or undergo dialysis are at high risk to MRSA exposure and infection.
Who is most at risk for a MRSA infection? +
MRSA infection affects certain populations disproportionately. Individuals with weakened immune systems, such as those living with HIV/AIDS, cancer, diabetes, young children, the elderly, those in contact with others who are in tight spaces like prisons or the military, or spend time in locker rooms, gyms or sports facilities are at risk due because of frequency of skin-to-skin contact. The elderly, blacks, and males have a higher incidence of MRSA than the general population.
What are the treatment options?Traditional antibiotic treatment options for MRSA have become more and more limited due to increased resistance. Vancomycin and comparable antibiotics remain the first line of defense. Recently, newer antimicrobial agents have been approved, offering physicians newer therapeutic options for treating this major public health problem.
What is the impact of MRSA? +
MRSA is a tremendous burden. It is estimated that there are 90,000 deaths a year.

About the Index
Matching Care Resources to Impacted Areas
The National Minority Quality Forum has developed a series of disease Atlases in keeping with its core vision “to eliminate health disparities through innovation, collaboration and evidence-based solutions.” These innovative internet-based disease atlases allow users to map disease incidence and prevalence, cost, outcomes, and multiple other variables at the zip-code-level. Atlases include, Diabetes, Chronic Kidney Disease, Cardiovascular Disease, HIV/AIDS, Peripheral Arterial Disease, Lung Cancer and the newest addition –methicillin-resistant Staphylococcus aureus (MRSA) – also known as the “super bug.” These Web-based maps provide users with a visual reference source to assess the impact of disease nationally, by state, by congressional district, and by state legislative district. Each Atlas allows users, including public health professionals, policy-makers, community leaders and individuals to look at data in a compelling way that complements existing information and data on a particular disease.
Mapping Diseases
For policy-makers and stakeholders, the atlases offer graphical displays of data that clearly shows geographic areas of impact, specific populations that are affected and an easy -to-understand way the impact of the disease in their jurisdiction or community so they can compare the impact of disease to other areas. The atlases provide a new way to look at data by layering in interactive features and illustrating data in a way that focuses on areas with the greatest need. The atlases were developed in close collaboration with George Washington University and utilize information and data from public databases and using propriety software. The maps are updated periodically as new data become available. The map projects are made possible through industry partnerships and are available to advocacy groups, policy makers, sponsoring organizations and individuals through a password-protected link from the Forum’s Web site.
Eliminating Health Disparities
The atlases are part of the Forum’s efforts to improve self-care, prevention, treatment, management, and monitoring and to eliminate health disparities and address the health care needs of the emerging majority. With an emphasis on utilizing data and the latest technology to understand and address health care issues, the Forum’s on the cutting edge of organizations pushing policy-makers and the medical community to look at and practice health care in a new, more data-driven manner. The present and future benefits of mapping diseases and other important, related information are more critical than ever in the effort to rein in rising health care costs.
See Additional MRSA Resources:
MRSA Atlas
http://www.mapmrsa.org
Centers for Disease Control
http://www.cdc.gov/mrsa/
WebMD
http://www.webmd.com/skin-problems-and-treatments/slideshow-closer-look-atmrsa?ecd=ppc_
Infectious Diseases Society of America
http://www.idsociety.org/
Executive Summary – MRSA Atlas
Mapping the “Super Bug”
Resource for the Front Lines
A Centers for Disease Control and Prevention (CDC) study, published in 2007, estimated that there were more than 94,000 infections by methicillin-resistant Staphylococcus aureus (MRSA) in the United States in 2005.[1] Infections varied by race/ethnicity, age, and gender, as well as geographically. In addition, published research indicates that invasive methicillin-resistant Staphylococcus aureus infections affect certain populations disproportionately as well as geographically. The elderly, blacks, and males are reported to have higher incidence of MRSA than the general population. As the epidemiology of infections with MRSA changes, a resource that can provide accurate information on the magnitude of MRSA infections in the US population is needed.
The introduction of the MRSA Atlas is designed to provide stakeholders and policymakers with a resource for estimating and mapping the number of hospital discharges associated with a primary or secondary diagnosis of MRSA (ICD-9-CM code V09.0) for every county in the United States. The data are derived from the Healthcare Cost and Utilization Project (HCUP) State Inpatient Database for 2006, state health departments, or from state synthetic estimates based on the national statistics for all stays through HCUPnet for 2006. For HCUP sourced data, zip code level estimates to determine the number of hospital discharges were calculated and mapped; further segmented by age (0–64; 65 years of age and older), gender, and race/ethnicity.
Key Findings
1. R. M. Klevens, M. A. Morrison, J. &#Nadle, S. Petit, K. Gershman, S. Ray, L. H. Harrison, R. Lynfield, G Dumyati, J. M. Townes, A. S. Craig, E. R. Zell, G. E. Fosheim, L. K. McDougal, R. B. Carey, S. K. Fridkin, and Active Bacterial Core surveillance (ABCs) MRSA Investigators, “Invasive Methicillin-Resistant Staphylococcus aureus Infections in the United States,” JAMA 298, no. 15 (2007): 1763–1771.
The Cost of MRSA
Reducing the incidence of MRSA in these communities has important economic ramifications as well. Costs associated with Staphylococcus aureus bloodstream infections for Medicare patients exceeded $2.5 billion in 2005. Hospital stays for MRSA infection have more than tripled since 2000, and have increased nearly ten-fold since 1995. Even if the infection does not require hospitalization, the prescription drug costs alone can average $1,000 for a ten-day regimen. Perhaps the most unnerving reality of MRSA is that, regardless of whether it is healthcare-associated or community-acquired, MRSA infections are largely preventable by improving the quality of the health care that is provided in hospitals, nursing homes and other facilities.
Objectives of the MRSA-QILC
To address the national problem of MRSA infections, the Forum is launching the MRSA Quality Improvement Learning Community (MRSA-QILC) to create an integrated framework for federal, state and local initiatives that are designed to prevent and/or reduce amenable morbidity and mortality linked to MRSA infections. Among its important objectives are:
- To increase support for the HHS Action Plan to Prevent Healthcare-Associated Infections as it relates specifically to achieving targets associated with Methicillin-resistant Staphylococcus Aureus (MRSA) infection. (HHS-APPHAI).
- To facilitate implementation of the MRSA components of the state plans that were submitted to CDC.
- To increase knowledge and awareness of key messages and prevention practices among providers, consumers, the media, and the general public. (HHS-APPHAI)
- To provide data and resources to support physician education efforts of National, State, and Local medical societies.
- To sponsor discussion forums about the MRSA challenge and effective health care and community interventions among elected officials, the leadership of state and local medical societies, hospital and health facility administrators, and key opinion leaders of affected communities.
- To increase awareness of community-specific incidence of MRSA in targeted geographic areas and to facilitate constructive collaborations around community-specific solutions.
- To increase knowledge and use of clinical guidelines for MRSA screening, prevention and treatment in both health care and community settings.
- To monitor, analyze and disseminate findings on community-specific MRSA reduction initiatives in targeted communities.